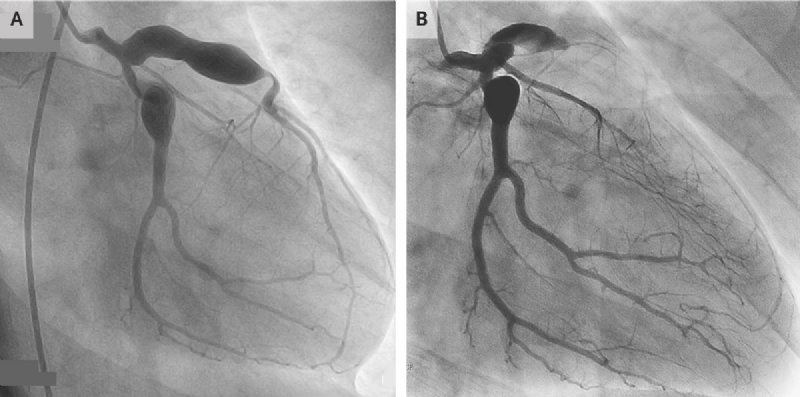
一18岁男孩因胸痛入急诊科接受治疗。该患11岁有川崎病史,尽管静脉注射免疫球蛋白,但影像呈现有冠状动脉瘤(A处为三年前冠脉血管造影影像),目前服用阿斯匹林和华法令。
An electrocardiogram showed ST-segment elevations in leads V1 to V3 Emergency coronary angiography revealed occlusion of the left anterior descending artery. Kawasaki’s disease is an acute, idiopathic, self-limiting vasculitis that primarily affects children. Clinical features include fever, nonexudative conjunctivitis in both eyes, mucositis,cervical lymphadenopathy, polymorphous rash, and changes in the hands and feet.
心电图显示V1 -3导联ST段抬高,急诊冠状动脉造影显示左前降动脉闭塞(图B)。川崎病是一种急性、先天性、自限性脉管炎,该病早期影响儿童。临床表现为发热、双眼非渗出性结膜炎、粘膜炎、颈椎淋巴结病、多型皮疹及手足改变等。
Because not all these features are necessarily present and there is no specific diagnostic test for Kawasaki’s disease, the diagnosis may be missed in childhood or occur at such an early age that the adult patient has no recollection of illness. Affected children are at risk for cardiovascular complications. The patient underwent coronary-artery bypass surgery. At follow-up 3 years after presentation, he was doing well and had no further cardiac symptoms.
因为以上特征不能都表现出来,而且对川崎病没有专门的诊断检验,儿童期忽略诊断,或早年发病,成年患者记不得有无既往史。患病儿童有心血管并发症的风险。该患接受了冠状动脉搭桥手术。术后随访3年,患者恢复良好,无其它心脏症状。